Science may be global, but access is still governed by power. Madhukar Pai reflects on vaccine inequity, India’s Delta wave, and why the future of health security depends on distributed manufacturing and fairer access.
The privilege of protection
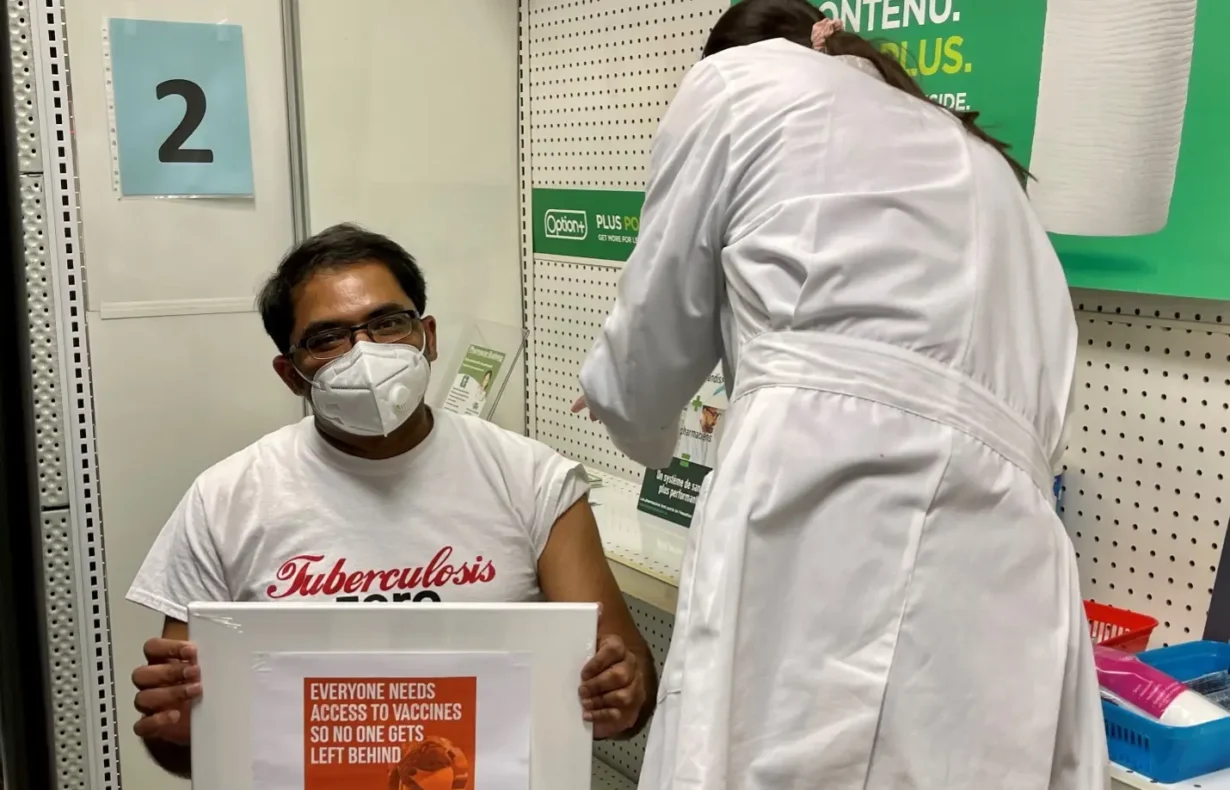
In April 2021, I was anxiously waiting for my turn to get my first COVID-19 vaccine shot. When my turn finally came and the Moderna vaccine went into my left shoulder, a wave of relief flooded my body. A huge weight was lifted. I knew then that, regardless of what came next, my body could fight the virus better. Even with one dose, I knew my ability to deal with the SARS-CoV-2 virus was dramatically enhanced.
My happiness was mixed with guilt. Even as I sat there getting vaccinated, I knew I was among the fortunate. Millions of people in the Global South had no access at that time. That contrast was impossible to ignore. Days after receiving my first dose, I wrote a piece outlining ten reasons why everyone should advocate for COVID-19 vaccine equity.
Science may be global, but its benefits are still distributed by power.
The lesson of India’s Delta wave
That same month in April 2021, India was slammed by the devastating Delta variant, which killed tens of thousands in a matter of weeks. My heart was heavy with the apocalyptic scenes of an entire nation gasping for oxygen. I spent those weeks trying to help friends and relatives over WhatsApp because they could not find timely medical care.
Watching my country’s health system implode was heartbreaking. It also clarified something that should have been obvious much earlier: a pandemic cannot be brought under control while lifesaving tools remain concentrated in a handful of countries. And without the protection of vaccines, SARS-CoV2 was a deadly virus.
If it was allowed to run through populations and countries, the result would be catastrophic. I co-authored an op-ed in the Washington Post about how India was an example to other countries. “If we do not heed this warning and work on vaccine equity, we risk a forever pandemic with long-term cycles of lockdowns, economic damage, and constant fear,” we wrote. I followed up with a piece entitled “Vax the world” in Science magazine.
Why access remained unequal
Five years later, we know exactly how things played out. The COVID-19 pandemic ended up disproportionately impacting the Global South, where vaccine coverage was poor or greatly delayed. Governments in the Global North secured early access to vaccine supplies on favorable terms while lower-income countries waited and waited. Global North governments hoarded vaccines and worked with pharmaceutical companies to block a waiver under the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), which could have enabled Global South countries to make their own mRNA vaccines during a period of dire need.
If vaccines had reached the Global South in an equitable and timely manner, half the deaths that occurred might have been averted. Even today, the mRNA technology remains largely a monopoly of Big Pharma. Manufacturing power remains concentrated. Access remains unequal.
Although vaccine inequity was a defining failure of the COVID-19 pandemic, inequitable access to medicines predates COVID-19. The pandemic merely exposed a deeper pattern in global health: lifesaving technologies too often reach poorer countries last, through systems designed around scarcity, hierarchy, and delayed access.
We had already seen this inequity with the struggle for anti-retroviral medicines for HIV, where it took nearly 2 decades of activism for the African region to get adequate access, with devastating consequences for the whole continent. Even after the COVID-19 pandemic, we saw inequities repeat themselves with access to mpox vaccines in Africa.
When systems are designed to repeatedly fail some groups, then racism is the key underlying driver of inequities, as I called out during the AIDS 2022 meeting in Montreal.
Beyond the trickle-down model
Science may be global, but its benefits are still distributed by power. So, how do we ensure that lifesaving products are not reserved for the elite and the privileged? How do we make sure science serves and saves all, not just some?
The good news is that alternative models already exist. We are no longer in a position where we must imagine what a fairer system might look like. We can already see parts of it emerging. Several strategies, outlined in the box, can be deployed to ensure equity in access to medicines and technologies.
Box: Strategies to improve equitable access to medicines and health technologies.
- All public investment, including tax-funded grants and contracts, should include global access licensing requirements.
- All publicly funded R&D should include clauses that allow intellectual property to be licensed to Global South manufacturers.
- Drugs funded with public money should come with a plan to ensure access in the countries where clinical trials are undertaken.
- Big Pharma should face stronger regulation, including price controls where appropriate, such as for insulin or COVID-19 vaccines.
- Competition should be increased through stronger support for generic production.
- The patent system should be overhauled to prevent abuse and gaming.
- The public sector should manufacture essential health goods where needed.
- Manufacturing should be diversified globally, with much greater production capacity in the Global South.
- Any pandemic accord should include enforceable provisions on equity and technology sharing.
Many of these strategies are already being used with good effect. For example, the state of California is now manufacturing insulin to make this century-old product more affordable. The public sector can and must manufacture lifesaving products, when private industry is unable or unwilling to.
Generic manufacturing is another proven strategy to increase access. The revolutionary long-acting HIV prevention drug, lenacapavir, will be available as a generic, at a cost of US$40 a year, in 120 low- and middle-income countries starting in 2027, manufactured under license by an Indian company. These are important signals. They show that affordability is often a question of political and industrial choice, not scientific impossibility.
There are equally important examples from the Global South itself. Products made in the Global South are already starting to make an impact. A Chinese-made near point-of-care molecular test for TB is now endorsed by WHO and available at a cost of $3.6 per test, about half the cost of established rapid molecular technologies.
India, which carries a major share of the global cervical cancer burden, has launched a nationwide HPV vaccinationcampaign and now produces its own HPV vaccine at a more affordable price point. Previously, India introduced Rotavac, an affordable, indigenous oral rotavirus vaccine through the Universal Immunization Program, with substantial protection against severe rotavirus disease.
In 2025, Bangladesh launched a nationwide typhoid conjugate vaccine campaign to protect millions of children, using doses developed by Indian companies and supplied through Gavi.
In Africa, the African Union has reaffirmed its commitment to local health product manufacturing, pooled procurement, and regulatory harmonization, aiming to meet at least 60% of the continent’s health product needs through local manufacturing by 2040. The Institut Pasteur de Dakar has developed the world’s first rapid diagnostic test for measles, now recommended for use within the Global Measles and Rubella Laboratory Network.
These examples matter because they challenge a tired assumption in global health: that innovation flows in one direction, manufacturing capacity belongs elsewhere, and poorer countries must wait for trickle-down access. That model was always inequitable. During COVID-19, it’s limits were fully exposed.
The Global South has already shown that it can innovate, manufacture, and invest in health technologies.
Building a fairer system
A fairer system will require several things at once: investment in local and regional R&D as well as manufacturing, technology transfer, stronger regulatory systems, pooled procurement, and sustained south-south cooperation. It will also require political confidence. Countries in the Global South do not need to remain permanently dependent on a model that has repeatedly failed them in moments of acute need.
That does not mean every country must make everything. It means the world must stop treating Big Pharma as the sole innovator, or concentrated manufacturing power in the Global North as natural, efficient, or inevitable when its consequences are so clearly unequal. Resilience comes from distributed capacity. Equity comes from designing systems that value timely access for all rather than protection for those who can pay a lot and bring profits for companies. And innovations are not a monopoly of the Global North.
COVID-19 gave us a brutal case study on what happens when lifesaving tools are treated as assets to be secured by the wealthy first and shared later as a charity. We should not need another catastrophe to absorb the core lesson. Charity is not justice.
The question now is whether we are prepared to act on what multiple pandemics have revealed. The Global South has already shown that it can innovate, manufacture, and invest in health technologies. What remains is the political will to build a different order: one in which science serves all, and one in which access to medicines and vaccines is a human right, not an act of charity.
Madhukar Pai is the Inaugural Chair of the Department of Global and Public Health at the McGill School of Population and Global Health. He holds a Tier 1 Canada Research Chair in Epidemiology and Global Health, and previously served as Director of the McGill International TB Center. He was the inaugural Editor-in-Chief of PLOS Global Public Health.