Three years ago, a 48-year-old man in Bubiashie, Accra, began to feel unwell. The signs were easy to dismiss at first: headaches, fatigue, dizziness, the kind of symptoms many people carry for longer than they should while life presses on. He was not in routine contact with care. By the time he finally sought help, hypertension had done its quieter work. What began as a manageable risk had become kidney failure. He died.
His story is personal. It is also recognizable and becoming far too common. Across Ghana, too many people still present to the health system late, after the early warning has passed, and treatment has become harder, costlier, and less forgiving. Ghana’s 2023 STEPwise survey found hypertension in 21.7 percent of adults aged 18 to 69, and 51.1 percent of those with elevated blood pressure had not previously been diagnosed.
A reform at the first point of care
That is the context in which Ghana’s free primary healthcare program should be judged. The program and the National Health Insurance Scheme serve different functions within the same health system. The National Health Insurance Scheme remains Ghana’s main platform for pooled financial protection and covers a broad benefits package, including outpatient and inpatient care and more than 95 percent of disease conditions.
The new program is trying to solve a different problem: delayed, uncertain, or financially difficult first contact with care, especially in underserved areas. The Presidency says the program will begin in 150 underserved districts and expand nationwide by 2028, and it has described the initiative as complementary to the National Health Insurance Scheme.
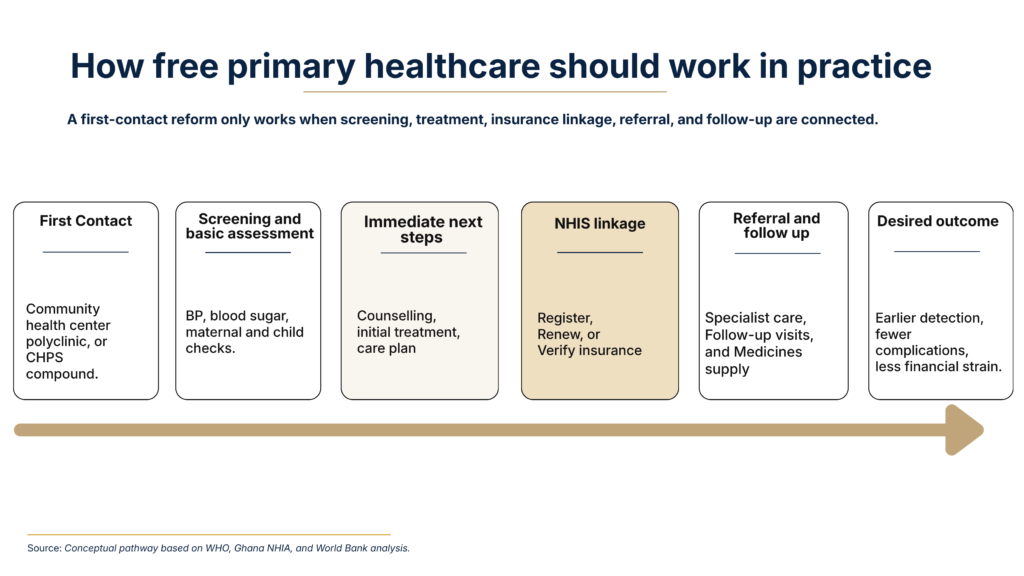
Primary health care failures begin quietly. They become visible later as stroke, kidney disease, diabetic complications, maternal risk, and household financial distress. The World Health Organization defines primary health care broadly, from health promotion and disease prevention to treatment, rehabilitation, and palliative care delivered as close as possible to where people live. Ghana’s initiative aims to strengthen that first point of contact before preventable risk hardens into crisis.
Why the policy case is strong
The policy logic behind the program is sound. Ghana carries a large burden of chronic disease risk that is still being detected too late. The STEPwise survey shows a high prevalence of elevated blood pressure and substantial undiagnosed disease. The same report notes that noncommunicable diseases account for about 45 percent of all deaths in Ghana. In a country with that disease profile, easier screening and earlier routine contact with care are not cosmetic improvements. They are basic system requirements.
The financing case is strong as well. The United Nations Children’s Fund Ghana 2025 health budget brief found that preventive care averaged only 12.3 percent of health expenditure from 2019 to 2023, while out-of-pocket spending averaged 27 percent of current health expenditure. The Ministry of Finance’s 2025 budget also uncapped the National Health Insurance Levy and allocated 9.93 billion Ghana cedis for the National Health Insurance Scheme, including claims payments, essential medicines, vaccines, free primary healthcare, and other health commitments. Ghana has therefore made a serious fiscal choice to move care closer to prevention and earlier access.
Where the reform could succeed or fail
The next task is clarity. A program called free primary healthcare creates a broad public expectation. People will reasonably assume consultation, diagnosis, medicines, and continuity of care. The government’s own public language, however, points to a program that still needs a clearer public definition. The Presidency has described routine screening, maternal and child health services, immunization, and treatment for common illnesses.
The National Health Insurance Authority has described a delivery model in which visits are validated through a One-Time Attendance Code generated with either a Ghana Card number or a National Health Insurance Scheme membership number, including expired cards. That is a useful operational detail. It is not yet the same thing as a simple public guarantee that households can understand without confusion.
Readiness matters just as much. The Ministry of Health says it has procured 24,534 pieces of equipment for the rollout, including basic diagnostic and clinical equipment. That is an important step. Still, equipment counts are not the same as service readiness. Readiness is a service platform: staff, medicines, diagnostics, referral links, and the ability to keep care moving once a patient enters the system. The question is whether each rollout district can carry the promise being made to citizens.
Continuity may prove to be the hardest test of all. The World Bank’s recent brief on noncommunicable disease care in Ghana found that 51.7 percent of patients reported visiting more than one facility for care. That figure points to fragmentation in the patient journey. A system can improve first contact and still lose patients in subsequent steps. Screening numbers may rise quickly. The reform will matter far more when abnormal findings lead to treatment, treatment leads to follow-up, and follow-up prevents avoidable deterioration.
A stronger front door is valuable. A coherent patient pathway is what turns access into health gain.
Four moves that would strengthen the program
First, the government should publish a short national guarantee in plain language. Citizens should not have to decode the program through speeches, radio panels, or facility discretion. They should be able to see, in one place, what is free at first contact, where it is available, what identification is accepted, what happens after referral, and where to report improper charges. That kind of clarity is not merely a communications exercise; it is what makes entitlement usable. Ghana’s own rollout materials already show how easily confusion can arise when a broad political promise meets a more specific operational model built around the Ghana Card, the National Health Insurance Scheme card, including expired cards, and a One-Time Attendance Code. A reform of this scale needs one public promise that households can understand and providers can apply consistently.
Second, Ghana should make free primary healthcare the strongest entry point yet into the National Health Insurance Scheme, not a parallel pathway beside it . This matters for continuity and sustainability. The National Health Insurance Authority says membership coverage reached 66 percent in 2025 and that it is targeting at least 80 percent by the end of 2026. If free primary healthcare becomes a screening gateway without a built-in path into the National Health Insurance Scheme, many patients will be detected early and then lost when they need repeat visits, medicines, diagnostics, or referral beyond the first-contact package. Every first-contact visit should therefore be used to register, renew, update, or reactivate coverage. No patient identified with hypertension, diabetes, pregnancy risk, or chronic illness should leave the first encounter as an administrative orphan.
Third, rollout should follow verified district readiness, not national excitement. The government is right to begin in underserved districts, and the equipment push is important. A fast rollout without a functioning service platform would weaken the reform at a moment when public expectations are highest. Expansion should be guided by evidence that each district has the minimum combination of staff, medicines, diagnostics, referral capacity, and fallback systems needed to consistently deliver the promise.
Fourth, the program should guarantee the first treatment step, not only the first test. Many health systems celebrate screening numbers and underdesign the care that follows an abnormal result. That is how a prevention reform becomes a detection campaign with limited clinical value. Ghana should define a short list of conditions for which the first response is guaranteed: confirmation, first-line medicines where appropriate, a written care plan, and a booked follow-up or confirmed referral. The World Bank’s findings on fragmented noncommunicable disease care show why this matters. The program will matter far more if it becomes known for catching patients early and keeping hold of them, not simply for identifying risk earlier.
The standard that matters
The central theme is straightforward. Ghana needs the National Health Insurance Scheme and free primary healthcare to work together. One supports financial protection across a broad package of care. The other has the potential to make first contact easier, earlier, and more reliable. If Ghana can connect those functions clearly and consistently, this initiative could become one of the country’s most important access reforms in years. If that connection remains loose, citizens will continue to feel the distance between policy language and lived experience.
That is the standard worth applying now. Can someone in the relatively urban community of Bubiashie or in any other community, urban or rural get screened before silent risk becomes a visible catastrophe? Can the system respond with medicines, follow-up, and referral before a manageable condition becomes a crisis? Can the government show, in public, that first contact with care is becoming easier and more reliable? Those are the questions that will decide whether this program becomes a durable gain in health policy or a promising idea that outran its delivery model.
Dr. William Nii Ayitey Menson is Director of Health Financing for Africa at ONE Campaign and a physician by training. He leads advocacy to boost domestic and international investment in health and has supported reforms, immunization, and COVID-19 responses across 20 countries on 4 continents. He previously worked at Gavi, CHAI, and McKinsey.
Dr. Banda Khalifa is a Ghanaian physician, epidemiologist, and global health strategist whose work spans evidence translation, health systems strengthening, and implementation across international and public-sector settings. He is the Founder and Editor-in-Chief of The Meridian Letters and has worked across WHO, the Tony Blair Institute, the United Nations, and public health agencies in the United States.